[ COVID Updated Guidelines ] Isolation and Precautions for People with COVID-19 ... CDC ends test-to-stay for schools and relaxes COVID rules
 CDC ends test-to-stay for schools and relaxes COVID rules
CDC ends test-to-stay for schools and relaxes COVID rules
Updated Aug. 11, 2022
https://www.cdc.gov/coronavirus/2019-ncov/your-health/isolation.htmlUpdated Aug. 11, 2022
https://www.cdc.gov/coronavirus/2019-ncov/your-health/isolation.html
---------------------------------
CDC ends test-to-stay for schools and relaxes COVID rules
August 11, 20223:19 PM ET
by Will Stone and Pien Huang
www.npr.org
With the coronavirus continuing to spread widely throughout the country, Americans are getting new advice from federal health officials on how to live with the virus.
The revised guidance – released by the Centers for Disease Control and Prevention on Thursday – lifts the requirement to quarantine if exposed to the virus, deemphasizes screening people with no symptoms and updates COVID-19 protocols in schools, eliminating a recommendation for test-to-stay after potential exposure.
"This guidance acknowledges that the pandemic is not over, but also helps us move to a point where COVID-19 no longer severely disrupts our daily lives," the CDC's Greta Massetti said in a statement. "We know that COVID 19 is here to stay," she added in comments during a briefing with reporters.
The update isn't necessarily a huge overhaul of the existing guidance, but it does represent an increasing focus on individuals making their own decisions about their level of risk and how they want to mitigate that risk, said Dr. Marcus Plescia, chief medical officer for the Association of State and Territorial Health Officials.
"That is consistent with where we are in the pandemic right now," he said. "I don't really think there are many state or local jurisdictions that are feeling they're going to need to start making mandates."
It also brings the recommendations for unvaccinated people in line with people who are fully vaccinated – an acknowledgment of the high levels of population immunity in the U.S., due to vaccination, past COVID-19 infections or both. "Based on the latest ... data, it's around 95% of the population," Massetti said, "And so it really makes the most sense to not differentiate," since many people have some protection against severe disease.
The changes could have some of the biggest impact in K-12 schools. The guidance eliminates the strategy known as "test-to-stay" – a schedule of testing for people that were exposed to the coronavirus but not up to date with their vaccinations – that allowed them to continue in-person learning, so long as they continued to test negative and showed no symptoms.
The test-to-stay protocol has been an alternative to quarantine for school, so now "the practice of handling exposures would involve masking rather than a quarantine," Massetti said.
https://www.npr.org/sections/health-shots/2022/08/11/1116991600/with-new-guidance-cdc-ends-test-to-stay-for-schools-and-relaxes-covid-rules
--------------------------------
Summary of Guidance for Minimizing the Impact of COVID-19 on Individual Persons, Communities, and Health Care Systems —
United States, August 2022
Early Release / August 11, 2022 / 71
Greta M. Massetti, PhD1; Brendan R. Jackson, MD1; John T. Brooks, MD1; Cria G. Perrine, PhD1; Erica Reott, MPH1; Aron J. Hall, DVM1; Debra Lubar, PhD1; Ian T. Williams, PhD1; Matthew D. Ritchey, DPT1; Pragna Patel, MD1; Leandris C. Liburd, PhD1; Barbara E. Mahon, MD1 (View author affiliations)
High levels of immunity and availability of effective COVID-19 prevention and management tools have reduced the risk for medically significant illness and death.
What is added by this report?
To prevent medically significant COVID-19 illness and death, persons must understand their risk, take steps to protect themselves and others with vaccines, therapeutics, and nonpharmaceutical interventions when needed, receive testing and wear masks when exposed, receive testing if symptomatic, and isolate for ≥5 days if infected.
What are the implications for public health practice?
Medically significant illness, death, and health care system strain can be reduced through vaccination and therapeutics to prevent severe illness, complemented by use of multiple prevention methods to reduce exposure risk and an emphasis on protecting persons at high risk for severe illness.
As SARS-CoV-2, the virus that causes COVID-19, continues to circulate globally, high levels of vaccine- and infection-induced immunity and the availability of effective treatments and prevention tools have substantially reduced the risk for medically significant COVID-19 illness (severe acute illness and post–COVID-19 conditions) and associated hospitalization and death (1). These circumstances now allow public health efforts to minimize the individual and societal health impacts of COVID-19 by focusing on sustainable measures to further reduce medically significant illness as well as to minimize strain on the health care system, while reducing barriers to social, educational, and economic activity (2). Individual risk for medically significant COVID-19 depends on a person’s risk for exposure to SARS-CoV-2 and their risk for developing severe illness if infected (3). Exposure risk can be mitigated through nonpharmaceutical interventions, including improving ventilation, use of masks or respirators indoors, and testing (4). The risk for medically significant illness increases with age, disability status, and underlying medical conditions but is considerably reduced by immunity derived from vaccination, previous infection, or both, as well as timely access to effective biomedical prevention measures and treatments (3,5). CDC’s public health recommendations change in response to evolving science, the availability of biomedical and public health tools, and changes in context, such as levels of immunity in the population and currently circulating variants. CDC recommends a strategic approach to minimizing the impact of COVID-19 on health and society that relies on vaccination and therapeutics to prevent severe illness; use of multicomponent prevention measures where feasible; and particular emphasis on protecting persons at high risk for severe illness. Efforts to expand access to vaccination and therapeutics, including the use of preexposure prophylaxis for persons who are immunocompromised, antiviral agents, and therapeutic monoclonal antibodies, should be intensified to reduce the risk for medically significant illness and death. Efforts to protect persons at high risk for severe illness must ensure that all persons have access to information to understand their individual risk, as well as efficient and equitable access to vaccination, therapeutics, testing, and other prevention measures. Current priorities for preventing medically significant illness should focus on ensuring that persons 1) understand their risk, 2) take steps to protect themselves and others through vaccines, therapeutics, and nonpharmaceutical interventions when needed, 3) receive testing and wear masks if they have been exposed, and 4) receive testing if they are symptomatic, and isolate for ≥5 days if they are infected.
Vaccines and Therapeutics To Reduce Medically Significant Illness
COVID-19 vaccination. COVID-19 vaccines are highly protective against severe illness and death and provide a lesser degree of protection against asymptomatic and mild infection (6). Receipt of a primary series alone, in the absence of being up to date with vaccination* through receipt of all recommended booster doses, provides minimal protection against infection and transmission (3,6). Being up to date with vaccination provides a transient period of increased protection against infection and transmission after the most recent dose, although protection can wane over time. The rates of COVID-19–associated hospitalization and death are substantially higher among unvaccinated adults than among those who are up to date with recommended COVID-19 vaccination, particularly adults aged ≥65 years (5,7). Emerging evidence suggests that vaccination before infection also provides some protection against post–COVID-19 conditions,† and that vaccination among persons with post–COVID-19 conditions might help reduce their symptoms (8). Continuing to increase vaccination coverage and ensuring that persons are up to date with vaccination are essential to preventing severe outcomes. Overall booster dose coverage in the United States remains low,§ which is concerning given the meaningful reductions in risk for severe illness and death that booster doses provide and the importance of booster doses to counter waning of vaccine-induced immunity. Public health efforts to expand reach and promote equitable access to vaccination have resulted in similar rates of primary series coverage across most racial and ethnic groups (9); however, racial and ethnic disparities in booster coverage have emerged (10). Supporting community partnerships and leveraging trusted sources of information must continue in order to eliminate persistent disparities and achieve equity in booster dose coverage, including through increasing education efforts and promotion of equitable vaccination outreach. Public health efforts need to continue to promote up-to-date vaccination for everyone, especially with vaccines targeting emerging novel variants that might be more transmissible or immune-evasive.
Preexposure prophylaxis. COVID-19 vaccine effectiveness against severe outcomes is lower in persons who are immunocompromised than in those who are not, and persons who are immunocompromised and have COVID-19 are at increased risk for intensive care unit admission and death while hospitalized, irrespective of their vaccination status (11,12). Preexposure prophylaxis with Evusheld¶ can help protect persons with moderate to severe immunocompromise who might not mount an adequate immune response after COVID-19 vaccination, as well as persons for whom COVID-19 vaccination is not recommended because of their personal risk for severe adverse reactions. In addition to early antiviral treatment if infected, persons who are moderately or severely immunocompromised can benefit from COVID-19 preexposure prophylactic medication to help prevent severe COVID-19 illness, as an adjunct to up-to-date vaccination for themselves and their close contacts, early testing, nonpharmaceutical interventions, and prompt access to treatment if they are infected.
Medications to treat COVID-19. Antiviral medications (Lagevrio [molnupiravir], Paxlovid [nirmatrelvir and ritonavir], and Veklury [remdesivir]) and monoclonal antibodies (bebtelovimab) are available to treat COVID-19 in persons who are at increased risk for severe illness,** including older adults, unvaccinated persons, and those with certain medical conditions†† (13). Antiviral agents reduce risk for hospitalization and death when administered soon after diagnosis. The federal Test to Treat initiative facilitates rapid, no-cost access to oral COVID-19 treatment for eligible persons who receive a positive SARS-CoV-2 test result.§§ Recent expansion of prescribing authority of Paxlovid to pharmacists intends to further facilitate access.¶¶ Continued efforts are needed to reduce racial and ethnic differences in receipt of monoclonal antibody therapies (14) and disparities in dispensing rates for oral antiviral prescriptions by community social vulnerability (15).
COVID-19 Prevention Strategies
Monitoring COVID-19 Community Levels to guide COVID-19 prevention efforts. Persons can use information about the current level of COVID-19 impact on their community to decide which prevention behaviors to use and when (at all times or at specific times), based on their own risk for severe illness and that of members of their household, their risk tolerance, and setting-specific factors. CDC’s COVID-19 Community Levels reflect the current effect of COVID-19 on communities and identify geographic areas that might experience increases in severe COVID-19–related outcomes, based on hospitalization rates, hospital bed occupancy, and COVID-19 incidence during the preceding period*** (1). Prevention recommendations based on COVID-19 Community Levels have the explicit goals of reducing medically significant illness and limiting strain on the health care system. At all COVID-19 Community Levels (low, medium, and high), recommendations emphasize staying up to date with vaccination, improving ventilation, testing persons who are symptomatic and those who have been exposed, and isolating infected persons. At the medium COVID-19 Community Level, recommended strategies include adding protections for persons who are at high risk for severe illness (e.g., use of masks or respirators that provide a higher level of wearer protection). At the high COVID-19 Community Level, additional recommendations focus on all persons wearing masks indoors in public and further increasing protection to populations at high risk.††† As SARS-CoV-2 continues to circulate, changes in COVID-19 Community Levels for a jurisdiction help signal when use of some prevention strategies should be discontinued or increased, based on an individual person’s level of risk for severe illness or that of their household or social contacts. The COVID-19 Community Levels provide a broad framework for public health officials and jurisdictions to use and adapt as needed based on local context by combining local information to assess the need for public health interventions.
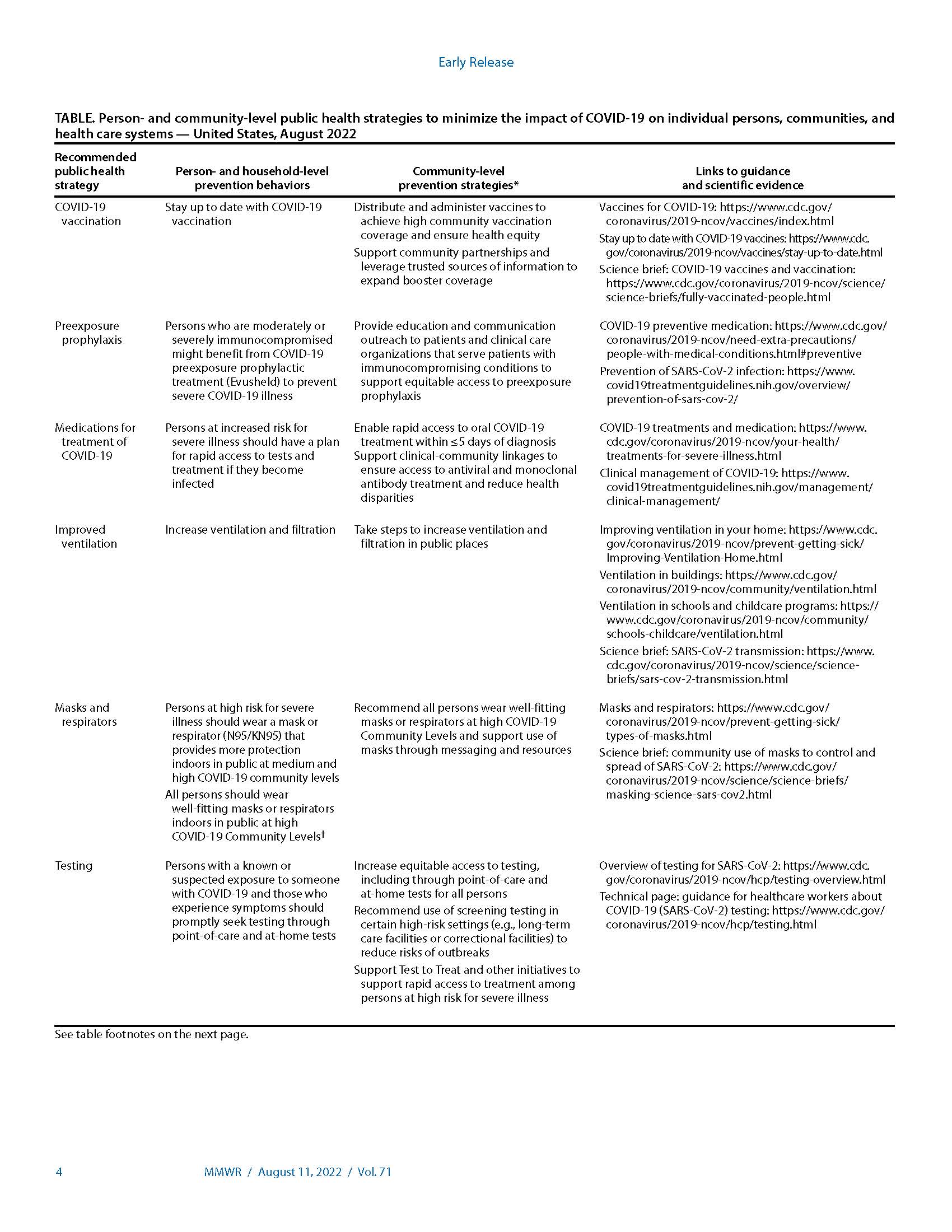
Nonpharmaceutical interventions. Implementation of multiple prevention strategies helps protect individual persons and communities from SARS-CoV-2 exposure and reduce risk for medically significant illness and death by reducing risk for infection (Table). Implementation of multiple nonpharmaceutical preventive interventions can complement use of vaccines and therapeutics, especially as COVID-19 Community Levels increase and among persons at high risk for severe illness. CDC’s COVID-19 prevention recommendations no longer differentiate based on a person’s vaccination status because breakthrough infections occur, though they are generally mild (16), and persons who have had COVID-19 but are not vaccinated have some degree of protection against severe illness from their previous infection (17). In addition to strategies recommended at all COVID-19 Community Levels, education and messaging to help individual persons understand their risk for medically significant illness complements recommendations for prevention strategies based on risk.
Testing for current infection. Diagnostic testing can identify infections early so that infected persons can take action to reduce their risk for transmitting virus and receive treatment, if clinically indicated, to reduce their risk for severe illness and death. All persons should seek testing for active infection when they are symptomatic or if they have a known or suspected exposure to someone with COVID-19. When considering whether and where to implement screening testing of asymptomatic persons with no known exposure, public health officials might consider prioritizing high-risk congregate settings, such as long-term care facilities, homeless shelters, and correctional facilities, and workplace settings that include congregate housing with limited access to medical care.§§§ In these types of high-risk congregate settings, screening testing might complement diagnostic testing of symptomatic persons by identifying asymptomatic infected persons (18,19). When implemented, screening testing strategies should include all persons, irrespective of vaccination status. Screening testing might not be cost-effective in general community settings, especially if COVID-19 prevalence is low (20,21).
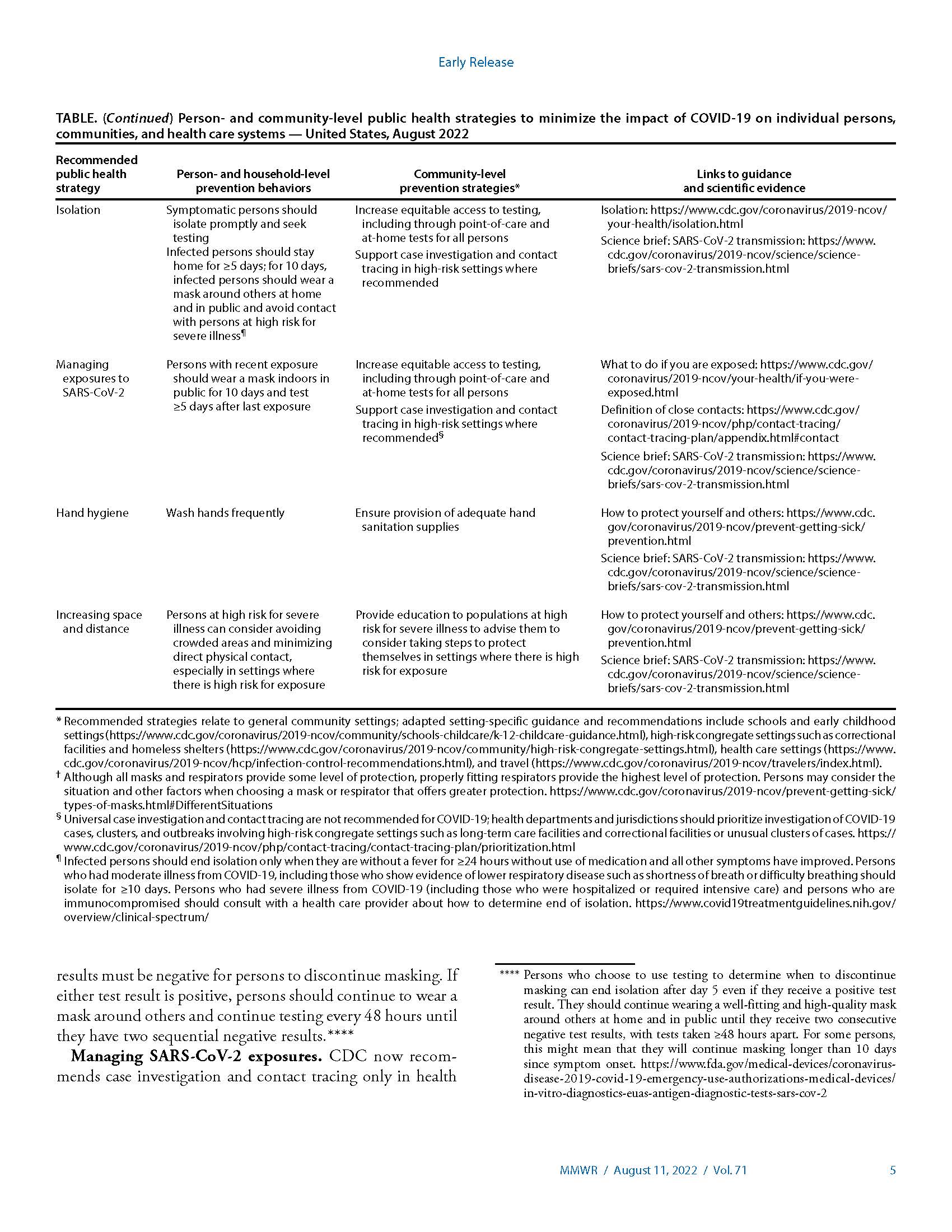
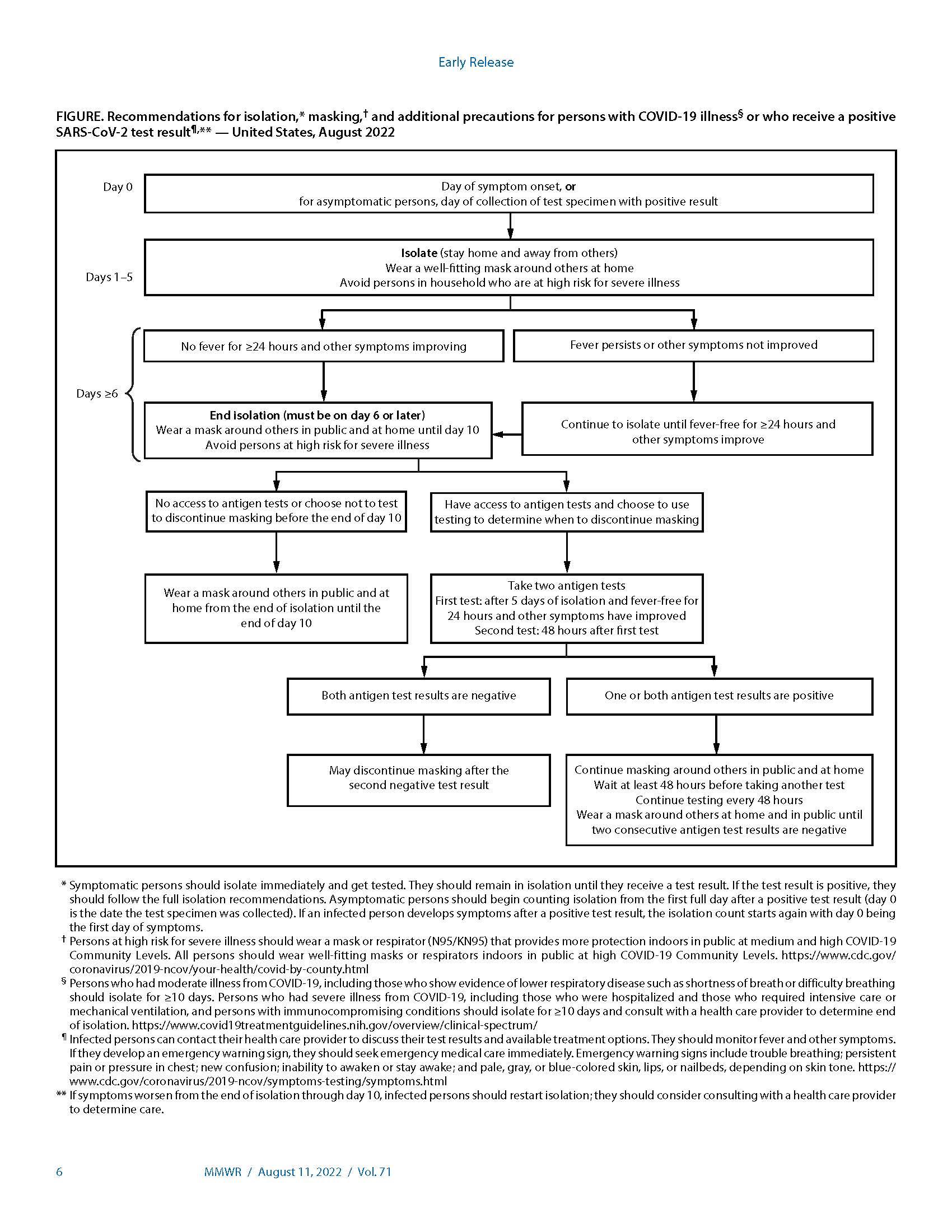
Isolation. Symptomatic or infected persons should isolate promptly, and infected persons should remain in isolation for ≥5 days and wear a well-fitting and high-quality mask or respirator if they must be around others. Infected persons may end isolation after 5 days, only when they are without a fever for ≥24 hours without the use of medication and all other symptoms have improved, and they should continue to wear a mask or respirator around others at home and in public through day 10¶¶¶ (Figure) (22,23). Persons who have access to antigen tests and who choose to use testing to determine when they can discontinue masking should wait to take the first test until at least day 6 and they are without a fever for ≥24 hours without the use of fever-reducing medication and all other symptoms have improved. Use of two antigen tests with ≥48 hours between tests provides more reliable information because of improved test sensitivity (24). Two consecutive test results must be negative for persons to discontinue masking. If either test result is positive, persons should continue to wear a mask around others and continue testing every 48 hours until they have two sequential negative results.****
Managing SARS-CoV-2 exposures. CDC now recommends case investigation and contact tracing only in health care settings and certain high-risk congregate settings.†††† In all other circumstances, public health efforts can focus on case notification and provision of information and resources to exposed persons about access to testing. Persons who have had recent confirmed or suspected exposure to an infected person should wear a mask for 10 days around others when indoors in public and should receive testing ≥5 days after exposure (or sooner, if they are symptomatic), irrespective of their vaccination status.§§§§ In light of high population levels of anti–SARS-CoV-2 seroprevalence (7,16), and to limit social and economic impacts, quarantine of exposed persons is no longer recommended, regardless of vaccination status.
Protecting Persons Most at Risk for Severe Illness
Multiple nonpharmaceutical and medical prevention measures are available to substantially reduce the risk for medically significant illness and death among persons at particularly high risk for these outcomes because of older age, disability, moderate or severe immunocompromise (25), or other underlying medical conditions (including pregnancy) (26). In addition to recommending that persons stay up to date with vaccination, public health strategies to protect persons at high risk include use of masks or respirators (i.e., specialized filtering masks such as N95/KN95s) that provide more protection for the wearer,¶¶¶¶ preexposure prophylaxis if indicated (e.g., for persons who are immunocompromised), and early access to and use of antivirals. At medium and high COVID-19 Community Levels, persons at high risk for severe illness and their contacts should consider wearing well-fitting masks or respirators that provide more protection to the wearer because of better filtration and fit to reduce exposure and infection risk. Persons who have household or social contact with persons at high risk should consider self-testing to detect infection before contact at medium and high COVID-19 Community Levels. Public health efforts should promote health equity by purposefully reaching out to all populations at high risk for severe illness to broaden access to preexposure prophylaxis, testing, and oral antivirals. Public health practitioners and organizations should consider the characteristics of their local or setting-specific populations when determining whether to strengthen or add prevention strategies that supplement disease control efforts and protect those persons at highest risk for severe illness or death. Strengthening public health communications and messaging can also help persons assess their personal level of risk for severe illness and use that knowledge to choose preventive behaviors to protect themselves and those around them.*****
Discussion
COVID-19 remains an ongoing public health threat; however, high levels of vaccine- and infection-induced immunity and the availability of medical and nonpharmaceutical interventions have substantially reduced the risk for medically significant illness, hospitalization, and death from COVID-19. As transmission of SARS-CoV-2 continues, the current focus on reducing medically significant illness, death, and health care system strain are appropriate and achievable aims that are supported by the broad availability of the current suite of effective public health tools. Rapid identification of emergent variants necessitating a shift in prevention strategy makes continued detection, monitoring, and characterization of novel SARS-CoV-2 variants essential. Incorporating actions to mitigate the impact of COVID-19 into long-term sustainable routine practices is imperative for society and public health.
Corresponding author: Greta M. Massetti, gmassetti@cdc.gov
https://www.cdc.gov/mmwr/volumes/71/wr/mm7133e1.htm?s_cid=mm7133e1_w
-------------
If you were exposed to COVID-19, you should start taking precautions.
https://www.cdc.gov/coronavirus/2019-ncov/your-health/isolation.html
This information is intended for a general audience. Healthcare professionals should see Ending Isolation and Precautions for People with COVID-19. This CDC guidance is meant to supplement—not replace—any federal, state, local, territorial, or tribal health and safety laws, rules, and regulations.
If you have COVID-19, you can spread the virus to others. There are precautions you can take to prevent spreading it to others: isolation, masking, and avoiding contact with people who are at high risk of getting very sick. Isolation is used to separate people with confirmed or suspected COVID-19 from those without COVID-19.
These recommendations do not change based on COVID-19 Community Levels. If you have COVID-19, also see additional information on treatments that may be available to you.
For Healthcare Professionals: Ending Isolation and Precautions for People with COVID-19
When to Isolate
Regardless of vaccination status, you should isolate from others when you have COVID-19. You should also isolate if you are sick and suspect that you have COVID-19 but do not yet have test results. If your results are positive, follow the full isolation recommendations below. If your results are negative, you can end your isolation.
IF YOU TEST
Negative
You can end your isolation
IF YOU TEST
Positive
Follow the full isolation recommendations below
When you have COVID-19, isolation is counted in days, as follows:
If you had no symptoms
Day 0 is the day you were tested (not the day you received your positive test result)
Day 1 is the first full day following the day you were tested
If you develop symptoms within 10 days of when you were tested, the clock restarts at day 0 on the day of symptom onset
If you had symptoms
Day 0 of isolation is the day of symptom onset, regardless of when you tested positive
Day 1 is the first full day after the day your symptoms started
Isolation
If you test positive for COVID-19, stay home for at least 5 days and isolate from others in your home. You are likely most infectious during these first 5 days.
Wear a high-quality mask if you must be around others at home and in public.
Do not go places where you are unable to wear a mask, including travel and public transportation settings.
Stay home and separate from others as much as possible.
Use a separate bathroom, if possible.
Take steps to improve ventilation at home, if possible.
Don’t share personal household items, like cups, towels, and utensils.
Monitor your symptoms. If you have an emergency warning sign (like trouble breathing), seek emergency medical care immediately.
Learn more about what to do if you have COVID-19.
Ending Isolation
End isolation based on how serious your COVID-19 symptoms were.
If you had no symptoms
You may end isolation after day 5.
If you had symptoms
You may end isolation after day 5 if:
You are fever-free for 24 hours (without the use of fever-reducing medication)
Your symptoms are improving
If you still have fever or your other symptoms have not improved, continue to isolate until they improve.
If you had moderate illness (if you experienced shortness of breath or had difficulty breathing), or severe illness (you were hospitalized) due to COVID-19-, or you have a weakened immune system, you need to isolate through day 10.
If you had severe illness or have a weakened immune system, consult your doctor before ending isolation. Ending isolation without a viral test may not be an option for you.
If you are unsure if your symptoms are moderate or severe or if you have a weakened immune system, talk to a healthcare provider for further guidance.
Regardless of when you end isolation, avoid being around people who are more likely to get very sick from COVID-19 until at least day 11. Remember to wear a high-quality mask when indoors around others at home and in public and not go places where you are unable to wear a mask until you are able to discontinue masking (see below).
Loss of taste and smell may persist for weeks or months after recovery and need not delay the end of isolation.
Removing Your Mask
After you have ended isolation, when you are feeling better (no fever without the use of fever-reducing medications and symptoms improving),
Wear your mask through day 10.
OR
If you have access to antigen tests, you should consider using them. With two sequential negative tests 48 hours apart, you may remove your mask sooner than day 10.
Note: If your antigen test results1 are positive, you may still be infectious. You should continue wearing a mask and wait at least 48 hours before taking another test. Continue taking antigen tests at least 48 hours apart until you have two sequential negative results. This may mean you need to continue wearing a mask and testing beyond day 10.
After you have ended isolation, if your COVID-19 symptoms recur or worsen, restart your isolation at day 0. Talk to a healthcare provider if you have questions about your symptoms or when to end isolation.
[1] As noted in the Food and Drug Administration labeling for authorized over-the-counter antigen tests, negative test results do not rule out SARS-CoV-2 infection and should not be used as the sole basis for treatment or patient management decisions, including infection control decisions.
Last Updated Aug. 11, 2022